|
|
Pheochromocytoma
General Considerations
- Rare, catecholamine-secreting, neuroendocrine tumor usually found in medulla of the adrenal gland originating in the chromaffin cells
- Extra-adrenal tumors called paraganglioneuromas
- Most often produces epinephrine and norepinephrine (mostly) which is unregulated by any feedback mechanism
- Sometimes dopamine is secreted
- About 10 % are malignant
- Occur at any age with peak in 3rd-5th decades, equal frequency in both sexes
- Locations of extra-adrenal pheochromocytomas include the organ of Zuckerkandl which is close to the origin of the inferior mesenteric artery, bladder wall, heart, mediastinum, and carotid and glomus jugulare bodies
Clinical Findings
- Headaches, palpitations and diaphoresis with hypertension, frequently episodic
- Weakness
- Nausea
- Tremors
- Anxiety
- Weight loss
- Plasma metanephrine measurements are most sensitive but have lower specificity
- Twenty-four hour urine collection for creatinine, total catecholamines, vanillylmandelic acid and metanephrine has a lower sensitivity but higher specificity
Imaging Findings
- Over 90% located in adrenal, 98% in abdomen
- Imaging studies are performed after the diagnosis is made on a biochemical basis
- MRI is the preferred study
- Hyperintense on T2-weighted images
- No contrast required
- CT scanning
- Most have a pre-contrast attenuation >10 HU
- Contrast was thought to add the risk of inducing hypertensive crisis but no increased risk has been shown with low-osmolar contrast
- Most lesions vigorously contrast-enhance (>80 HU) and have less than 60% washout of contrast on delayed images
- PET scans have also proved helpful in finding the lesions
Differential Diagnosis
- Adrenal adenomas
- Adrenal carcinomas
- Adrenal metastases
Associations
- Von-Hippel Lindau disease
- Neurofibromatosis
- Multiple endocrine neoplasia (MEN) 2A (Sipple syndrome) and 2B
- Tuberous sclerosis
- Sturge-Weber syndrome
Treatment
- Surgical resection of the mass is the treatment of choice
- Medical treatment is generally used pre-operatively, for management of the hypertensive crises and for treating metastatic disease, if present
Complications
- Cardiac arrhythmias
- Pulmonary edema
- Dilated cardiomyopathy
- Hypertensive encephalopathy
- Stroke


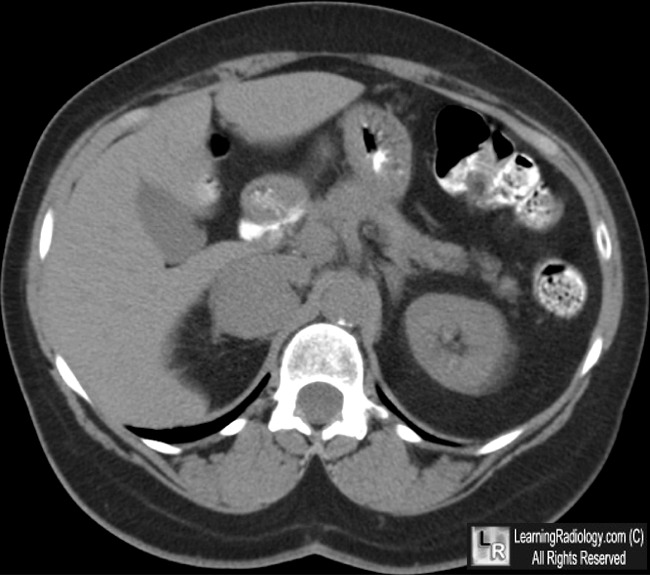
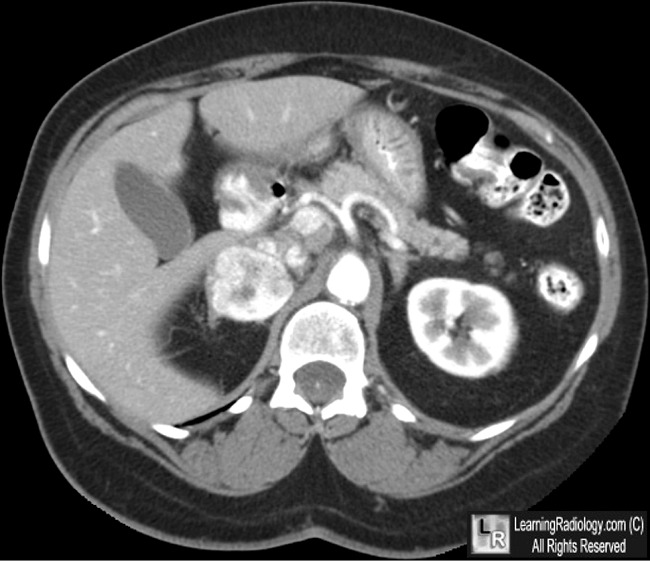
Pheochromocytoma. Pre-contrast axial CT of abdomen shows a mass in the right adrenal gland (white arrow)
The left adrenal gland is normal (yellow arrow). Following intravenous contrast (lower photo),
the right adrenal mass enhances brightly (red arrow).
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
eMedicine: Pheochromocytoma. AT Sweeney and MA Blake
Adrenocortical Carcinomas and Adrenal Pheochromocytomas: Mass and Enhancement loss Evaluation at Delayed Contrast-enhanced CT. Radiology 2005; 234:479 – 485. DH Szolar; M Korobkin; P Reittner; A Berghold; T Bauernhofer; H Trummer; H Schoellnast; KW. Preidler; H Samonig
|
|
|

{kind=link}
{kind=link}